17.1 Physical Characteristics of Urine
Learning Objectives
By the end of this section, you will be able to:
- Compare and contrast blood plasma, glomerular filtrate, and urine characteristics
- Describe the characteristics of a normal urine sample, including normal range of pH, osmolarity, and volume
The urinary system’s ability to filter the blood resides in about 2 to 3 million tufts of specialised capillaries—the glomeruli—distributed more or less equally between the two kidneys. Because the glomeruli filter the blood based mostly on particle size, large elements like blood cells, platelets, antibodies, and albumen are excluded. The glomerulus is the first part of the nephron, which then continues as a highly specialised tubular structure responsible for creating the final urine composition. All other solutes, such as ions, amino acids, vitamins, and wastes, are filtered to create a filtrate composition very similar to plasma. The glomeruli create about 200 litres of this filtrate every day, yet you excrete less than two litres of waste per day of urine.
Characteristics of the urine vary, depending on influences such as water intake, exercise, environmental temperature, nutrient intake, and other factors (Table 17.1.1.). Some of the characteristics such as colour and odour are rough descriptors of your state of hydration, for example, if you exercise or work outside, and sweat a great deal, your urine will turn darker and produce a slight odour, even if you drink plenty of water. Athletes are often advised to consume water until their urine is clear. This is (mostly) good advice; however, it takes time for the kidneys to process body fluids and store it in the bladder. Another way of looking at this is that the quality of the urine produced is an average over the time it takes to make that urine. Producing clear urine may take only a few minutes if you are drinking a lot of water or several hours if you are working outside and not drinking much.
Table 17.1.1. Normal urine characteristics
| Characteristic | Normal values |
| Colour | Pale yellow to deep amber |
| Odour | Odourless |
| Volume | 750-2000mL/24h |
| pH | 4.5-8.0 |
| Specific gravity | 1.003-1.0032 |
| Osmolarity | 40-1350 mOsmol/kg |
| Urobilinogen | 0.2-1.0 mg/100mL |
| White blood cells | 0-2 HPF (per high-power field of microscope) |
| Leukocyte esterase | None |
| Protein | None or trace |
| Bilirubin | <0.3 mg/100mL |
| Ketones | None |
| Nitrites | None |
| Blood | None |
| Glucose | None |
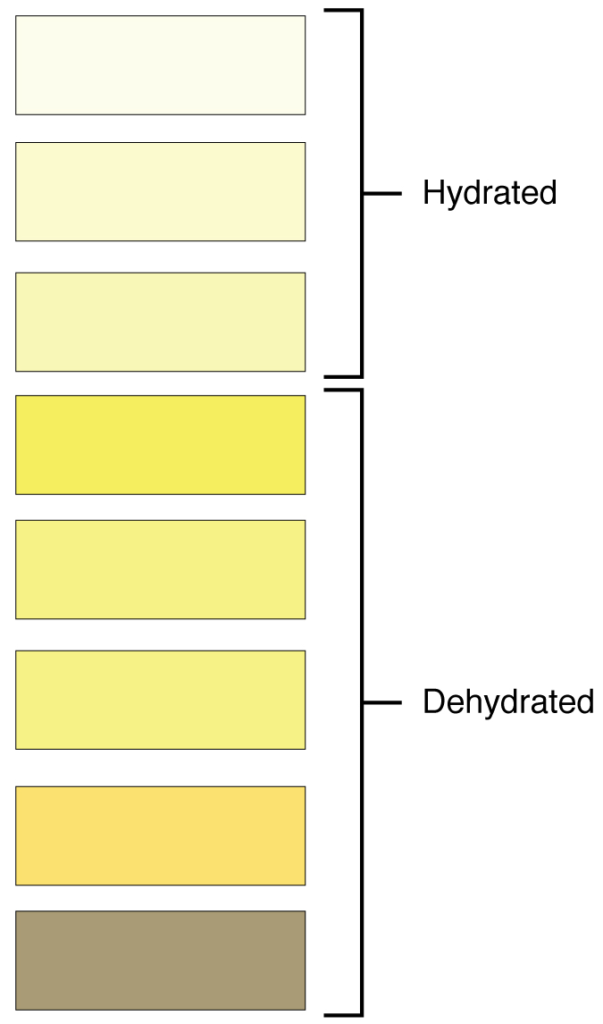
Urinalysis (urine analysis) often provides clues to renal disease. Normally, only traces of protein are found in urine, and when higher amounts are found, damage to the glomeruli is the likely basis. Unusually large quantities of urine may point to diseases like diabetes mellitus or hypothalamic tumours that cause diabetes insipidus. The colour of urine is determined mostly by the breakdown products of red blood cell destruction (Figure 17.1.1). The “haem” of haemoglobin is converted by the liver into water-soluble forms that can be excreted into the bile and indirectly into the urine. This yellow pigment is urochrome. Urine colour may also be affected by certain foods like beets, berries and fava beans. A kidney stone or a cancer of the urinary system may produce sufficient bleeding to manifest as pink or even bright red urine. Diseases of the liver or obstructions of bile drainage from the liver impart a dark “tea” or “cola” hue to the urine. Dehydration produces darker, concentrated urine that may also possess the slight odour of ammonia. Most of the ammonia produced from protein breakdown is converted into urea by the liver, so ammonia is rarely detected in fresh urine. The strong ammonia odour you may detect in bathrooms or alleys is due to the breakdown of urea into ammonia by bacteria in the environment. About one in five people detect a distinctive odour in their urine after consuming asparagus; other foods such as onions, garlic and fish can impart their own aromas! These food-caused odours are harmless.
Urine volume varies considerably. The normal range is one to two litres per day (Table 17.1.2). The kidneys must produce a minimum urine volume of about 500 mL/day to rid the body of wastes. Output below this level may be caused by severe dehydration or renal disease and is termed oliguria. The virtual absence of urine production is termed anuria. Excessive urine production is polyuria, which may be due to diabetes mellitus or diabetes insipidus. In diabetes mellitus, blood glucose levels exceed the number of available sodium-glucose transporters in the kidney and glucose appears in the urine. The osmotic nature of glucose attracts water, leading to its loss in the urine. In the case of diabetes insipidus, insufficient pituitary antidiuretic hormone (ADH) release or insufficient numbers of ADH receptors in the collecting ducts means that too few water channels are inserted into the cell membranes that line the collecting ducts of the kidney. Insufficient numbers of water channels (aquaporins) reduce water absorption, resulting in high volumes of very dilute urine.
Table 17.1.2. Urine volumes
| Volume condition | Volume | Causes |
| Normal | 1-2 L/day | |
| Polyuria | >2.5 L/day | Diabetes mellitus; diabetes insipidus; excess caffeine or alcohol; kidney disease; certain drugs, such as diuretics; sickle cell anaemia; excessive water intake |
| Oliguria | 300-500 mL/day | Dehydration; blood loss; diarrhoea; cardiogenic shock; kidney disease; enlarged prostate |
| Anuria | <50 mL/day | Kidney failure; obstruction, such as kidney stone or tumour; enlarged prostate |
The pH (hydrogen ion concentration) of the urine can vary more than 1000-fold, from a normal low of 4.5 to a maximum of 8.0. Diet can influence pH; meats lower the pH, whereas citrus fruits, vegetables and dairy products raise the pH. Chronically high or low pH can lead to disorders, such as the development of kidney stones or osteomalacia.
Specific gravity is a measure of the quantity of solutes per unit volume of a solution and is traditionally easier to measure than osmolarity. Urine will always have a specific gravity greater than pure water (water = 1.0) due to the presence of solutes. Laboratories can now measure urine osmolarity directly, which is a more accurate indicator of urinary solutes than specific gravity. Remember that osmolarity is the number of osmoles or milliosmoles per litre of fluid (mOsmol/L). Urine osmolarity ranges from a low of 50–100 mOsmol/L to as high as 1200 mOsmol/L H2O.
Cells are not normally found in the urine. The presence of leukocytes may indicate a urinary tract infection. Leukocyte esterase is released by leukocytes; if detected in the urine, it can be taken as indirect evidence of a urinary tract infection (UTI).
Protein does not normally leave the glomerular capillaries, so only trace amounts of protein should be found in the urine, approximately 10 mg/100 mL in a random sample. If excessive protein is detected in the urine, it usually means that the glomerulus is damaged and is allowing protein to “leak” into the filtrate.
Ketones are by-products of fat metabolism. Finding ketones in the urine suggests that the body is using fat as an energy source in preference to glucose. In diabetes mellitus when there is not enough insulin (Type I diabetes mellitus) or because of insulin resistance (Type 2 diabetes mellitus), there is plenty of glucose, but without the action of insulin, the cells cannot take it up, so it remains in the bloodstream. Instead, the cells are forced to use fat as their energy source, and fat consumed at such a level produces excessive ketones as by-products. These excess ketones will appear in the urine. Ketones may also appear if there is a severe deficiency of proteins or carbohydrates in the diet.
Nitrates (NO3–) occur normally in the urine. Gram-negative bacteria metabolise nitrate into nitrite (NO2–), and its presence in the urine is indirect evidence of infection.
There should be no blood found in the urine. It may sometimes appear in urine samples as a result of menstrual contamination, but this is not an abnormal condition. Now that you understand what the normal characteristics of urine are, the next section will introduce you to how you store and dispose of this waste product and how you make it.
Section Review
The kidney glomerulus filters blood mainly based on particle size to produce a filtrate lacking cells or large proteins. Most of the ions and molecules in the filtrate are needed by the body and must be reabsorbed farther down the nephron tubules, resulting in the formation of urine. Urine characteristics change depending on water intake, exercise, environmental temperature, and nutrient intake. Urinalysis analyses characteristics of the urine and is used to diagnose diseases. A minimum of 400 to 500 mL urine must be produced daily to rid the body of wastes. Excessive quantities of urine may indicate diabetes insipidus or diabetes mellitus. The pH range of urine is 4.5 to 8.0 and is affected by diet. Osmolarity ranges from 50 to 1200 milliosmoles and reflects the amount of water being recovered or lost by renal nephrons.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
